Trick or Treatment: One More Trick Played by Tumor Uncovered
The search for cancer treatment has arguably been the biggest challenge for biomedical research for decades. We all know that cancer is a big deal. Major advancements were made - we found that our immune system has mechanisms to fight cancerous cells.1 Yet, at least in some cases, our immunity fails to defend us. We also found that cancerous cells manage to evade and/or suppress immune responses.1,2 Ever since this finding, one of the major directions for cancer immunotherapy research is finding ways to counter cancer immunosuppression so that immune system can clear the tumor in our bodies. The reason why it is not as easy as it seems is that we do not fully understand all the ‘tricks’ cancerous cells pull off to suppress immune responses. In this post, I am going to talk about a research by Chen et al. (2018)3 which unmasks one other way cancers do it and sheds light to some of the important questions.
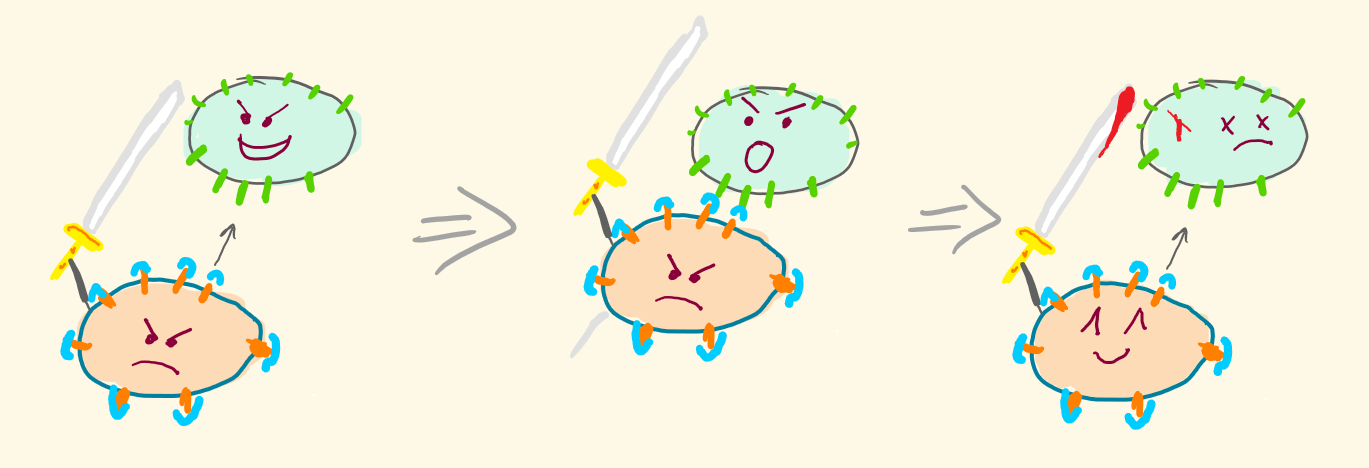
One of the major players in an immune system that kills cancer cells is Cytotoxic T cell (CD8+ T cells), a type of white blood cells. Unfortunately for us, many cancer types, including metastatic melanoma (a type of skin cancer) upregulate a transmembrane protein PD-L1 on their cell surface.4 This protein binds to PD-1, a transmembrane protein on T cells, and through this binding inactivates/ induces apoptosis in CD8+ T cells.5

In normally functioning tissues, PD-L1 and other ligands for PD-1 are used by our bodies when we need to dampen down our immune response.6 This is one way we evade autoimmune responses.6 However, cancerous cells use this mechanism to their advantage and effectively evade the immune response.
Once this was found, a promising idea for a new cancer immunotherapy was born. Researchers thought that blocking PD-1 on T cells by anti-PD-1 antibodies (Pembrolizumab) would prevent PD-L1 - PD-1 binding, allowing T cells to survive and target and destroy cancer cells.4
The research showed remarkable promise in treating metastatic melanoma with pembrolizumab treatment, however, the patient response rate was low.7 Chen et al. (2018) try to look into it closely and uncover missing parts in our understanding of the system that would explain the failure of the treatment.
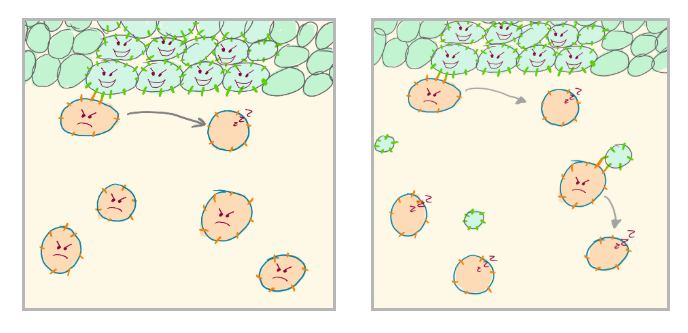
Researchers knew that cell-derived extracellular vesicles like exosomes are present in eukaryotic fluids, carry important bioactive molecules and, most importantly, influence the extracellular environment and immune system.8 So they decided to study exosomes in metastatic melanoma cell lines in hopes of understanding whether exosomes could be involved in immune evasion. Interestingly, by quantifying the amount of PD-L1-specific binding to isolated exosomes, they found that exosomes are significantly denser with PD-L1 in metastatic melanoma cell lines than in healthy control lines.3 Most likely, this is another technique used by cancerous cells that plays a role in immune evasion. In addition to expressing PD-L1 surface proteins on their membranes, they deploy exosomal vesicles with PD-L1 too to increase exposure of T cells to PD-L1 and suppress immunity globally in the body without the need of a direct contact with T cells.
Interestingly, an exosomal PD-L1 expression is increased with the increase of IFN-gamma, a molecule released indicative of T cell activity.3 It almost seems like tumors have a mechanism to react correspondingly to increased immune activity by reinforcing their defense mechanism. To see whether exosomal PD-L1 is truly involved in immune evasion in live organisms, they observed tumor growth in mice that could not produce PD-L1 themselves under different conditions. They injected one group of mice with exosomes that contained PD-L1 and observed significantly faster growth of the tumor than control.3 Tumor in mice that were injected with exosomes that were pre-treated with anti-PD-1 antibodies, however, did not grow as much.3 Chen et al. suggest that exosomal PD-L1 does suppress anti-tumor immunity and that this activity can be disrupted to some degree by PD-L1 blocking antibodies.3 Additionally, through microscopy, Chen et al. have shown that exosomes and CD8 T cells do interact physically.3 Even though exosomal PD-L1 clearly leads to the increased size of the tumor in this mice, I think additional experiments would have made their claim that PD-L1 does play a role in immune evasion more convincing. We do not know how exosomal PD-L1 injection will affect the size of the tumor in mice that can produce functional PD-L1 in tumor tissues like normal mice would do. Their claim does sound logical, however, they have not disproved the possibility of exosomal PD-L1 mediated inactivation of T cell response being futile in the presence of PD-L1 on cancerous tissue. However, it is understandable that experimental limitations often constrain scientists to perform experiments with minimal intervention.
To see whether this feature of PD-L1 expression in exosomes is linked to pembrolizumab treatment failure, they measure pretreatment levels of exosomal PD-L1 in patients. They found that pretreatment levels of exosomal PD-L1, as well as of IFN-gamma were significantly higher in patients who failed to responded to the anti-PD-1 antibody treatment.3 What this means we do not know for sure! It might suggest that exosomal PD-L1 levels determine the success of the treatment but we do not yet have enough evidence to claim a clear causal relationship between the two. In fact, it is probably unlikely, because anti-PD-1 antibodies should be as effective against exosomal PD-L1 activity as they are against PD-L1 on tumor tissue since they block the receptor (PD-1) on the T cells. Researchers of this study suggest that in patients with low exosomal PD-L1 levels, pembrolizumab treatment indirectly upregulates T cell function (activity peaked at 3 weeks). This leads to more IFN-gamma production which leads to more exosomal PD-L1 production by cancer cells (peaked at 6 weeks). However, the interaction between PD-1 and PD-L1 is blocked by pembrolizumab and therefore PD-L1 production is futile and ineffective.3 Therefore, T cell clears the tumor successfully. Whereas, in non-responder patients, high pretreatment PD-L1 levels might be indicative of production of large amounts of IFN-gamma due to prolonged T cell activity. Prolonged T cell activity probably led to an exhaustion of T cell population to the point that their reinvigoration is impossible even with anti-PD-1 treatment.3 As of now, we have no evidence to support or reject this hypothesis.
Even though this research group has not uncovered the full picture of why pembrolizumab treatment is not as successful as we expected, they show that exosomal PD-L1 is involved in immune response evasion. Most importantly, however, from now on, pretreatment levels of exosomal PD-L1 can potentially be used as a good indicator to predict (to a limited extent) the outcome of the treatment.3 Low exosomal PD-L1 in a patient would be an indication of a higher chance of success and vice versa. This blood-based pretreatment indicator now can be used to assess the viability of pembrolizumab treatment in advance so that they are administered more effectively.
This finding is one example of how biological research has direct implications for healthcare. Additionally, this research now opens up different directions of research that would increase the effectiveness of the pembrolizumab treatment. I think, one of the most important questions that need to be addressed is whether there are some patterns in the dynamics of exosomal PD-L1 levels. If so then we can probably time the treatment better to increase effectiveness. Furthermore, can we somehow regulate the PD-L1 blood concentration or decrease IFN-gamma levels in patients through external manipulations? If so, then can we design a pretreatment preparation for patients that would increase the treatment success rate? Can we revive the exhausted T cell population in patients? Answers to these questions, as well as uncovering all the ‘tricks’ cancerous cells rely on to evade the immune system will get us even closer to viable treatment(s) over cancer.
Disclaimer: Figures are not meant to be scientifically accurate.
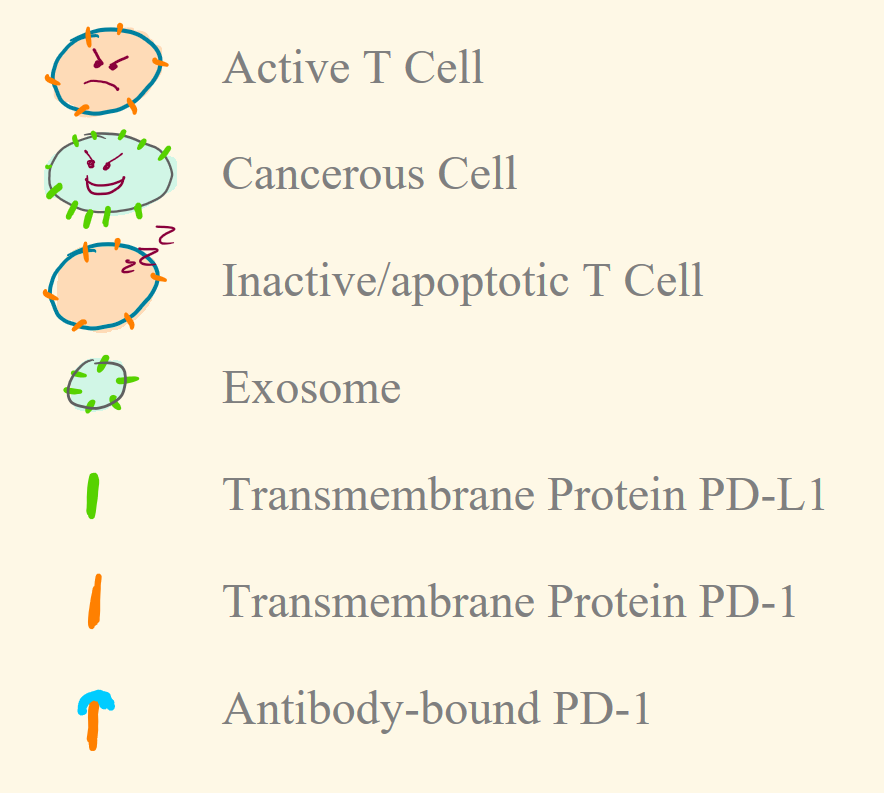
Legend for the figures:
Paper Reviewed
Chen, G., Huang, A., Zhang, W., Zhang, G., Wu, M., Xu, W., . . . Guo, W. (2018). Exosomal PD-L1 contributes to immunosuppression and is associated with anti-PD-1 response. Nature, 560(7718), 382-382.
References
1) Leskowitz, S., Phillipino, L., Hendrick, G., & Graham, J. B. (1957). Immune response in patients with cancer. Cancer, 10(6), 1103-1105.
2) Seliger, B. (2005). Strategies of tumor immune evasion. Biodrugs, 19(6), 347-354.
3) Chen, G., Huang, A., Zhang, W., Zhang, G., Wu, M., Xu, W., . . . Guo, W. (2018). Exosomal PD-L1 contributes to immunosuppression and is associated with anti-PD-1 response. Nature, 560(7718), 382-382.
4) Chen, L., & Han, X. (2015). Anti-PD-1/PD-L1 therapy of human cancer: Past, present, and future. Journal of Clinical Investigation, 125(9), 3384-3391.
5) Shi, F., Shi, M., Zeng, Z., Qi, R., Liu, Z., Zhang, J., . . . Wang, F. (2011). PD‐1 and PD‐L1 upregulation promotes CD8+ T‐cell apoptosis and postoperative recurrence in hepatocellular carcinoma patients. International Journal of Cancer, 128(4), 887-896.
6) Francisco, L., Sage, P., & Sharpe, A. (2010). The PD-1 pathway in tolerance and autoimmunity. Immunological Reviews, 236, 219-242.
7) Ribas, A., Hamid, O., Daud, A., Hodi, F. S., Wolchok, J. D., Kefford, R., . . . Robert, C. (2016). Association of pembrolizumab with tumor response and survival among patients with advanced melanoma. Jama, 315(15), 1600-1609.
8) Kalluri, R. (2016). The biology and function of exosomes in cancer. Journal of Clinical Investigation, 126(4), 1208-1215.
No comments:
Post a Comment