In response to: Schubert, R. D., Hawes, I. A., Ramachandran, P. S., Ramesh, A., Crawford, E. D., Pak, J. E., ... & Lyden, A. (2019). Pan-viral serology implicates enteroviruses in acute flaccid myelitis. Nature medicine, 1-5.
Over the past seven years, a polio-like disease called pediatric acute flaccid myelitis (AFM) has plagued children in the United States in increasing numbers. The first case of AFM was reported in California in 2012, but since then, there have been over 500 reported cases across the United States (Ayscue et al., 2014). The symptoms of AFM include weakness in the arms and legs, difficulty breathing, and internal lesions to the child’s spinal cord (Sejvar et al., 2016). While many children who develop AFM can survive the infection, very few children are able to make a full recovery; as a result, most afflicted children must live with permanent limb and respiratory disabilities (Sejvar et al., 2016). Currently, medical researchers and neurological pediatricians do not know what causes the disease, so understanding why this debilitating disease manifests is of critical importance to the medical community.
While the cause of the disease is unknown at this time, epidemiological research, which looks at broad trends in public health and diseases to make connections in regards health-related questions, has linked AFM to two strains of enterovirus, EV-D68 and EV-A71. Enteroviruses are single-stranded positive-sense RNA viruses and are a genus of virus from the Picornaviridae virus family. Strains of enterovirus are the causative agents for a variety of diseases ranging from the common cold to the poliovirus. The EV-A71 strain of the enterovirus has been associated with a spectrum of neurological diseases while the EV-D68 strain has been primarily found in children suffering from respiratory illnesses such as pneumonia or bronchiolitis (Brown et al., 2018). In 2014, spikes in AFM cases in the United States were found in areas that also had increased rates of EV-D68 and EV-A71 infection (Aliabadi et al., 2016). While the epidemiological research has demonstrated an association between both AFM and EV-D68 and EV-A71, no studies have been able to produce results that would indicate a causal relationship between either strain of the enterovirus and AFM. To determine a causal relationship between a virus and a disease, researchers generally look for the presence of either viral nucleic acid or viral antibodies in the patients’ cerebral spinal fluid (CSF). The presence of either molecule in a person’s CSF indicates that the person’s immune system is either actively fighting the virus or has previously encountered that virus. Previous research, however, has found that only two percent of AFM patients have detectable levels of enterovirus nucleic acid in their CSF. These findings have caused some scientists in the medical community to question whether enterovirus infection is the cause of AFM (Messacar et al., 2016). To demonstrate whether or not the enterovirus is the main trigger for AFM, researchers at the University of California, San Francisco performed a large scale search for viral antibodies in the CSF of patients with AFM to determine whether there is any biological evidence of a relationship between enteroviruses and AFM.
To discover which type of viruses could be linked to the development of AFM, the researchers examined the CFS of forty-two patients with AFM and fifty-eight healthy controls. Researchers screened for viral antibodies and viral nucleic acids in the CSF of both subject groups using several bioinformatics programs. These programs can be used to identify molecules in the subjects’ CSF through genome sequencing. A metagenomics next-generation sequencing (mNGS) was performed on the CFS of both the controls and the AFM patients to detect the presence of viral RNA. During the mNGS, nucleotides retrieved from the CSF of the patients and the controls were sequenced to a high degree of specificity and compared to the library of previously sequenced microorganisms and viral RNA. Following the mNGS sequencing, only one of the children with AFM tested positive for EV-A71 RNA and none of the children tested positive for EV-D68 RNA. The researchers’ results were consistent with earlier studies that had failed to find significant levels of enterovirus RNA in the CSF of children with AFM (Messacar et al., 2016).
After the viral RNA sequencing failed to demonstrate any relationship between enteroviruses and AFM, the researchers directed their attention to screening for antibodies in the patients’ CSF. Following infection, humans’ immune systems produce antibodies to target the infection. An antibody is an immune protein that specifically targets individual pathogens for they have antigen-binding sites that only attach to one type of antigen peptides that is created by solely the antibody’s target. The presence of a specific viral antibody in a patient’s CSF indicates a previous infection with the virus. Thus, although the researchers were unable to find evidence linking AFM to enterovirus infection when searching for elevated levels of enterovirus RNA, if enterovirus antibodies were found in the CSF of AFM patients the virus could still potentially be the causative agent of the disease.
To detect viral antibodies, the researchers utilized VirScan sequencing which uses bacteriophages that display viral peptides on their exterior to determine whether there are elevated levels of any viral antibody in a subject’s CSF. The VirScan program has 481,966 unique peptide sequences that can be used to identify vertebrate, mosquito-borne and tick-borne viral sequences. If the bacteriophage expressing a particular viral peptide is encountered by an antibody for the virus, the antibody will bind to the bacteriophage and the computer program which analyzes that data will signal a positive hit for the virus. The VirScan results showed that when compared with the CSF of healthy controls, the CSF of children with AFM had elevated levels of Picornaviridae peptides, the virus family to which the enteroviruses belong. When the Picornavirididae peptides were further examined, the greater levels of enrichment were almost entirely due to increased levels of enterovirus antibodies (Figure 1). The researchers also found that protein sequences common to enterovirus were elevated in the AFM patients’ CSF when compared with the controls’ CSF. For example, levels of viral protein 1 (VP1), a viral capsid protein predominately expressed by enteroviruses, were elevated in the CSF of AFM patients when compared to healthy controls (Figure 2).


Figure 1. Quantification of Enterovirus Enrichment in the CSF of Healthy Controls and AFM Cases. Following VirScan sequencing, the levels of enterovirus enrichment and the number of patients with enriched levels of enterovirus were quantified using a violin plot. The black dashed line represents the mean proportion of reads of enterovirus in the CSF and the red dotted line demarcates the third and first quartile for the proportion of reads of enterovirus. The width of the plot increases when more subjects who test positive. The greater the height of the violin plot indicates a greater proportion of positive reads in the subjects. Of the 42 AFM cases, 29 (69%) of the cases tested positive for EV antibodies. Of the 58 healthy controls, 4 (7%) of the controls tested positive for EV antibodies. There was a significant difference in the number of subjects in the two groups with the enterovirus antibodies in their CSF.
Following the VirScan search, the researchers performed an enzyme-linked immunosorbent assay (ELISA) to further assess whether enterovirus antibodies were upregulated in AFM patients. In an ELISA, antigens of interest are stuck to the bottom of plastic laboratory wells and then fluid containing a possible antibody, which for these experiments was the CSF of the AFM patients and the controls, is placed in the wells. If an antibody that binds to the antigen is present in the fluid added to the wells, the antibody will stick to the antigen and will not be removed from the plate when the nonspecific antibodies are washed away. Fluorescent substrates are then added to the wells and the amount of fluorescence in each well is used to quantify the level of antibody present in the cells. Greater levels of fluorescence in the wells indicate there were higher levels of the well antigen’s antibody present in the fluid added to the well. The researchers at the University of California, San Francisco used the VP1 protein as their well antigen and ran the ELISA with the CSF from the AFM patients and the healthy controls. Again, the researchers found that the CSF of AFM patients had elevated levels of enterovirus antibodies when compared with healthy controls. Also, AFM patients who had previously tested negative for enterovirus antibodies in the VirScan sequencing tested positive for enterovirus antibodies in the ELISA. This discrepancy in identification between the two assay calls into question the validity of VirScan for detecting enterovirus antibodies, suggesting that the researchers need to evaluate whether or not VirScan is an appropriate technique for enterovirus infection. In both the VirScan sequencing and ELISA, researchers did not find that one strain of enterovirus was predominately expressed in the CSF of patients with AFM. Researchers found that the CSF of AFM patients tested positive for multiple strains of enterovirus which indicates that co-infection with multiple strains of enterovirus might be necessary for the development of AFM, or a person who develops AFM may be more susceptible to additional infection of enteroviruses.

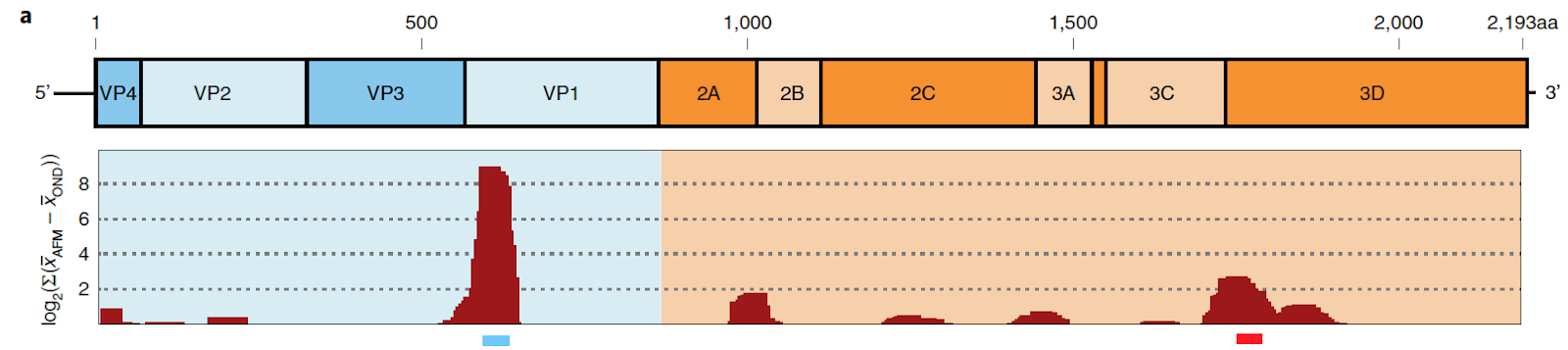
Figure 2. Enterovirus Enrichment at Specific Genome Sites in EV-A71 in the CSF of Healthy Controls and AFM Cases. Following VirScan sequencing, enterovirus-derived peptides found to be enriched in the CSF of AFM patients were plotted on genome sequence for different strains of enterovirus. The figure above demonstrates the enrichment of specific peptides found in the EV-A71 strain of the enterovirus. The BLASTp computer program was used to match viral peptides with their appropriate site in the EV-71A genome. The larger red peaks display greater enrichment of viral peptides in AFM patients when compared with healthy controls. Peptides such as VP1 were found to be significantly enriched in AFM patient’s CSF when compared to controls’ CSF.
Ultimately, the work completed by researchers at the University of California, San Francisco has provided another crucial link in establishing the relationship between enterovirus and AFM. The presence of elevated levels of enterovirus antibody in the CSF of AFM-afflicted children provides strong evidence to support that a causal relationship exists between enterovirus infection and the development of AFM. Moreover, the research shows that the detection of enterovirus antibodies in suspected patients’ CSF can be used as a diagnostic tool for identifying cases of AFM. While the work of the researchers at the University of California, San Francisco provides support for the theory that enterovirus causes AFM, more research needs to be completed before a causal link between enteroviruses and AFM is established. First, the study design of the researchers needs to be improved. The controls used for this study were significantly older than the AFM patients. The average age of the AFM patients was 38 months whereas the average age for the controls was 120 months. The age difference between the two groups presents a potential confounding variable that may have misconstrued the study results. Additionally, cohort studies, where healthy children are followed and evaluated to see which children become infected with the enterovirus, AFM, or both enterovirus and AFM, need to be completed to further determine whether or not a causal relationship exists between the two viruses for such studies allow researchers to establish a temporal relationship between the infection and the development of the disease. The proposed study would cost a significant amount of money so greater resources from agencies such as the Center for Disease Control would need to be directed towards AFM research.
AFM researchers also need to explain why enterovirus RNA cannot be detected in the CSF of AFM patients. Failure to account for why AFM patients do not present with elevated levels of enterovirus RNA in their CSF creates a major obstacle for demonstrating a causal relationship between enterovirus infection and the development of AFM. Lastly, AFM researchers should focus on uncovering a mechanism that explains how enterovirus infections result in the development of the neuro-motor deficits seen in patients with AFM. Overall, a significant amount of research needs to be completed to definitively link enterovirus infection to AFM, but the recent work completed at the University of California, San Francisco indicates that significant advances are being made in the medical community to identify the cause of this debilitating neurological disease. For further reading on the human cost of AFM infection, Pam Belluck, a reporter for the New York Times, recently detailed the experience of families with children who have developed AFM in this compelling article.
References:
Aliabadi, N., Messacar, K., Pastula, D. M., Robinson, C. C., Leshem, E., Sejvar, J. J., … Dominguez, S. R. (2016). Enterovirus D68 Infection in Children with Acute Flaccid Myelitis, Colorado, USA, 2014. Emerging infectious diseases, 22(8), 1387–1394. doi:10.3201/eid2208.151949
Ayscue, P., Van Haren, K., Sheriff, H., Waubant, E., Waldron, P., Yagi, S., … Centers for Disease Control and Prevention (CDC) (2014). Acute flaccid paralysis with anterior myelitis - California, June 2012-June 2014. MMWR. Morbidity and mortality weekly report, 63(40), 903–906.
Brown, D. M., Hixon, A. M., Oldfield, L. M., Zhang, Y., Novotny, M., Wang, W., … Scheuermann, R. H. (2018). Contemporary Circulating Enterovirus D68 Strains Have Acquired the Capacity for Viral Entry and Replication in Human Neuronal Cells. mBio, 9(5), e01954-18. doi:10.1128/mBio.01954-18
Messacar, K., Schreiner, T. L., Van Haren, K., Yang, M., Glaser, C. A., Tyler, K. L., & Dominguez, S. R. (2016). Acute flaccid myelitis: A clinical review of US cases 2012- 2015. Annals of neurology, 80(3), 326–338. doi:10.1002/ana.24730
Sejvar, J. J., Lopez, A. S., Cortese, M. M., Leshem, E., Pastula, D. M., Miller, L., … Feikin, D. (2016). Acute Flaccid Myelitis in the United States, August-December 2014: Results of Nationwide Surveillance. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 63(6), 737–745. doi:10.1093/cid/ciw372
AFM researchers also need to explain why enterovirus RNA cannot be detected in the CSF of AFM patients. Failure to account for why AFM patients do not present with elevated levels of enterovirus RNA in their CSF creates a major obstacle for demonstrating a causal relationship between enterovirus infection and the development of AFM. Lastly, AFM researchers should focus on uncovering a mechanism that explains how enterovirus infections result in the development of the neuro-motor deficits seen in patients with AFM. Overall, a significant amount of research needs to be completed to definitively link enterovirus infection to AFM, but the recent work completed at the University of California, San Francisco indicates that significant advances are being made in the medical community to identify the cause of this debilitating neurological disease. For further reading on the human cost of AFM infection, Pam Belluck, a reporter for the New York Times, recently detailed the experience of families with children who have developed AFM in this compelling article.
References:
Aliabadi, N., Messacar, K., Pastula, D. M., Robinson, C. C., Leshem, E., Sejvar, J. J., … Dominguez, S. R. (2016). Enterovirus D68 Infection in Children with Acute Flaccid Myelitis, Colorado, USA, 2014. Emerging infectious diseases, 22(8), 1387–1394. doi:10.3201/eid2208.151949
Ayscue, P., Van Haren, K., Sheriff, H., Waubant, E., Waldron, P., Yagi, S., … Centers for Disease Control and Prevention (CDC) (2014). Acute flaccid paralysis with anterior myelitis - California, June 2012-June 2014. MMWR. Morbidity and mortality weekly report, 63(40), 903–906.
Brown, D. M., Hixon, A. M., Oldfield, L. M., Zhang, Y., Novotny, M., Wang, W., … Scheuermann, R. H. (2018). Contemporary Circulating Enterovirus D68 Strains Have Acquired the Capacity for Viral Entry and Replication in Human Neuronal Cells. mBio, 9(5), e01954-18. doi:10.1128/mBio.01954-18
Messacar, K., Schreiner, T. L., Van Haren, K., Yang, M., Glaser, C. A., Tyler, K. L., & Dominguez, S. R. (2016). Acute flaccid myelitis: A clinical review of US cases 2012- 2015. Annals of neurology, 80(3), 326–338. doi:10.1002/ana.24730
Sejvar, J. J., Lopez, A. S., Cortese, M. M., Leshem, E., Pastula, D. M., Miller, L., … Feikin, D. (2016). Acute Flaccid Myelitis in the United States, August-December 2014: Results of Nationwide Surveillance. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 63(6), 737–745. doi:10.1093/cid/ciw372
No comments:
Post a Comment