Original Paper: Pathological significance of urinary complement activation in diabetic nephropathy: a full view from the development of the disease
Diabetes is a serious disease that results in elevated blood sugar levels. Blood glucose is a primary source of energy that comes from our food, and insulin is the key hormone that helps glucose enter cells to be used for energy. Common types of diabetes include Type 1 and Type 2, which occurs when the body produces too little insulin (Type 1) or is unable to use insulin efficiently (Type 2). The National Diabetes Statistic Report (2017) found that as of 2015, 30.3 million Americans (9.4% of the U.S. population) have diabetes, and another 84.1 million have pre-diabetes. This signifies a growing health problem, as diabetes was the seventh leading cause of death in the U.S. in 2015. Diabetes also comes with several serious health implications. More specifically, diabetic nephropathy (DN), or diabetic kidney disease, is a complication that affects approximately 25-30% of diabetics. DN ultimately results in chronic loss of kidney function, and it is the leading cause of renal disease worldwide (National Diabetes Statistic Report, 2017). These are alarming statistics, and they make research about the underlying mechanisms of DN ever so necessary.
The image below provides a general overview of how diabetic nephropathy contributes to kidney malfunction:
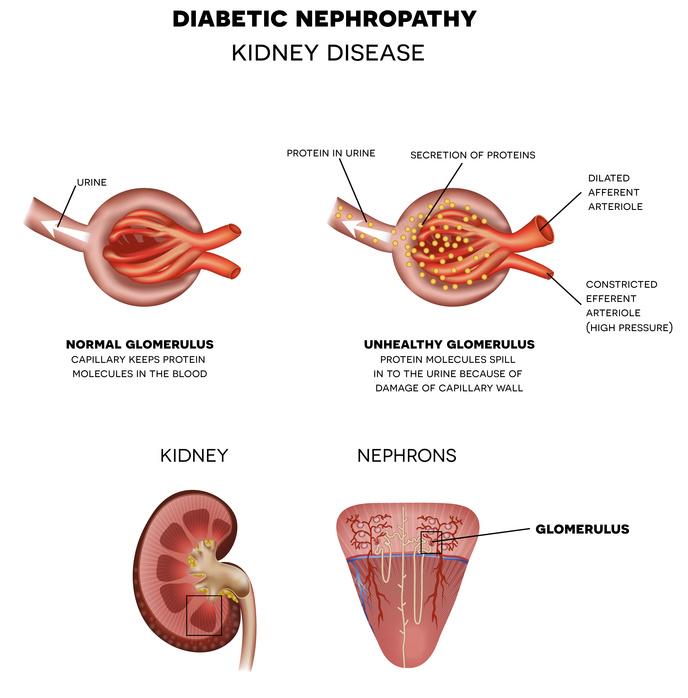 |
| https://www.rsnhope.org/health-library/nephropathy-diabetes-kidney-disease/attachment/diabetic-nephropathy-kidney-disease/ |
There are currently no therapeutic options to treat diabetic nephropathy. While the development of DN is understood to be multiplex, its exact consequences and underlying biological mechanisms are not completely understood. Previous studies suggest that complement may be involved in DN development, as increased urinary complement activation products (CAPs) have been reported in kidney diseases (including DN).
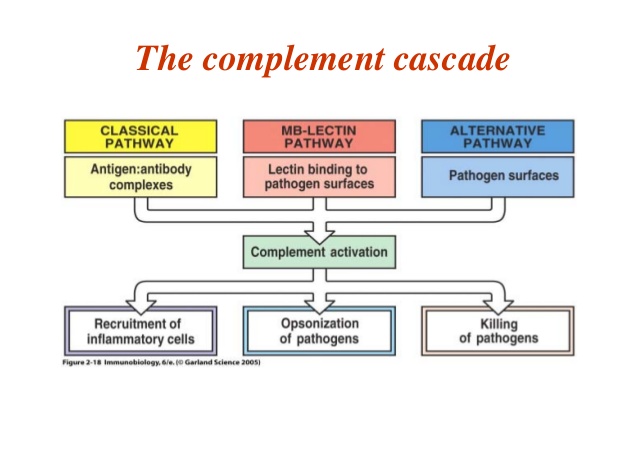
To break this all down: the complement system is a complex biochemical cascade that, when activated, “complements” the ability of antibodies to clear disease-producing agents from the body. The system consists of numerous proteins that are either directly involved in complement pathways or have other regulatory functions. Complement activation can occur through a variety of pathways, as seen below:
 |
| https://image.slidesharecdn.com/thecomplementsystem-052506-150321011504-conversion-gate01/95/the-complement-system-10-638.jpg?cb=1426901327 |
 |
| https://slideplayer.com/slide/5256405/ |
To understand the significance of urinary CAPs in relation to diabetic nephropathy, Dr. Jing-Ming Zheng and her lab at Taizhou Hospital considered CAP levels in patients at different stages of DN. They considered patients of different stages because DN is a diverse disease, so the impact of complement activation may differ depending on the stage. This is a huge strength of the study; it is comprehensive in its consideration of urinary CAPs in patients with all types of DN. It is also an advance from previous studies that primarily focused on advanced stages of DN.
The sample size of the study consisted of an experimental group of 62 type 2 DN patients. It also utilized two control groups: 20 type 2 diabetes patients without DN, and 20 healthy individuals. The DN patient group was further divided based on stage of disease, which was determined on the basis of certain clinical and histologic features. Urine and plasma samples were obtained and purified, and the samples were then analyzed for CAPs (C3a, C5a, C5b-9) through various microscopy and staining techniques. More specifically, urinary CAPs were measured through levels of urinary creatine in the samples.
The sample size of the study consisted of an experimental group of 62 type 2 DN patients. It also utilized two control groups: 20 type 2 diabetes patients without DN, and 20 healthy individuals. The DN patient group was further divided based on stage of disease, which was determined on the basis of certain clinical and histologic features. Urine and plasma samples were obtained and purified, and the samples were then analyzed for CAPs (C3a, C5a, C5b-9) through various microscopy and staining techniques. More specifically, urinary CAPs were measured through levels of urinary creatine in the samples.
Interestingly, Zheng et. al found that urinary CAP levels increase along with the progression of DN. That is, the worsening of a patient’s DN correlates with increases in the patient's urinary CAP levels (Figure 1). Also, no significant changes in urinary CAPS were observed in the control diabetic and normal groups. This supports that urinary CAPs play a role in the progression of diabetic nephropathy.
 |
| Figure 1. Urinary levels of C3a, C5a and C5b-9 in patients at different clinical stages of diabetic nephropathy. Higher CAP levels are evident in patients with more progressive DN. NG= normal control group, DMG= diabetes mellitus group (without nephropathy), MG= microalbuminuria stage group, PG= proteinuria stage group, RIG= renal insufficiency stage group. |
No significant changes in plasma CAP levels were observed, and DN patients had comparable levels of plasma CAPs to the two control groups. This suggests that plasma CAPs do not play a significant role in the development of DN. Also, there was no significant correlation between levels of urinary and plasma CAPs. So, increases in CAP levels with DN progression likely results from localized complement activation rather than from circulating complement activation (considering that plasma circulates throughout the whole body whereas the urinary tract is limited to a specific part in the body). These results also support the involvement of urinary CAPs in DN progression.
Lastly, Zheng et. al explored the relationship between urinary complement activation and physical kidney damage. To do this, renal biopsies were obtained from DN patients. More specifically, the DN group was further divided based on levels of urinary C3a. A positive correlation was ultimately observed: patients with higher C3a levels usually had more severe renal tubular damage. The lab also performed a series of statistical analyses and found that above-median levels of urinary CAPs were strongly associated with higher renal tubular damage. This remained the case even after the consideration of confounding factors.
So... we know that urinary CAPs play a role in DN. Now, we may know what this role actually is: CAPs could possibly contribute to (or, maybe directly cause) renal tubular damage. Based on their findings, Zheng et al. suggest that upon activation, CAPs exert harmful effects on tissues, perhaps through direct attack of complement proteins on cell surfaces. In sum, this study has shown a close correlation between urinary CAPs and stage of DN. The authors describe this direct correlation as a vicious cycle: Kidney damage > enhanced urinary complement activation > production of more urinary CAPs > CAPs filter through injured tubules (while also acting on vasculature) > further kidney damage > worsening DN.
The present study is significant in providing evidence of the role of CAPs in progressing DN and associated tubular damage. This is really important to understand the underlying mechanisms of diabetic nephropathy, which in turn could provide vital insight in combatting renal diseases associated with diabetes. An understanding of the biological origins of DN could be the first step towards the discovery of a drug that could provide specific, targetted interventions. For example, the more we understand the circular interplay between CAPs and DN progression, the closer we get to discovering treatments that could inhibit this cycle. This could lead to a hampering, or even complete prevention of renal diseases associated with diabetes. To help this happen, I think future directions could include focusing on other specific urinary CAPs and if they contribute to renal insufficiency in the same manner. Also, while this study is monumental in its broader consideration of DN as a disease, a broader sample size could be helpful in further validating the current findings, as this study only had 62 patients total, with only 20 being a variety of DN patients. Even adding a control group of non-diabetic patients with kidney failure would be interesting... this could help us understand whether the involvement of urinary CAPs is specific to diabetic kidney failure, or if it is involved in kidney diseases in general. This would give the study even broader implications, helping people with all different kinds of chronic kidney failure. Also, this is a stretch, but it would be interesting to study complement- deficient patients, how that contributes to their response to infection, and ultimately what this implicates for the "vicious cycle" between urinary CAPs and kidney disease. As the incidence of diabetes increases, it becomes increasingly important to understand the mechanisms of the complications they bring.
References:
1. Molitch ME, Adler AI, Flyvbjerg A, et al. Diabetic kidney
disease: a clinical update from Kidney Disease: improving
global outcomes. Kidney Int 2015; 87: 20–30.
4. Ghosh P, Sahoo R, Vaidya A, et al. Role of complement and
complement regulatory proteins in the complications of
diabetes. Endocr Rev 2015; 36: 272–288.
No comments:
Post a Comment